Note: This is mostly an updated version of a post of mine from last May, when it looked as though Senate Republicans were going to include "funding CSR reimbursement payments" as part of their Big Ugly Bill (officially the "One Big Beautiful Bill Act") which, among many other terrible things, included gutting Medicaid and didn't include extending the ACA's enhanced premium tax credits beyond December 2025.
Thankfully, in the end the Senate GOP didn't include the CSR funding provision...but House Republicans did include it in a bill which they passed last winter...which then died in the Senate since it would have required 60 votes there to move forward.
Next up: Age brackets, gender, racial/ethnic groups and urban/rural communities. I'm also throwing in the stand-alone Dental Plan table here for the heck of it since I don't know where else to include it.
Nationally, there hasn't been that much of a shift in the enrollment breakout by age bracket...but within each bracket there's a couple of takeaways:
As expected given the subsidy expiration, enrollment among young adults plummeted (down 7.4% & 8.5% among 18-25 yr olds & 26 - 34 yr olds respectively). This will absolutely have a disproportionate negative impact on the risk pool (and, thus, gross premiums) next year
On the other hand, enrollment of children actually increased by 3.4% year over year, which I wasn't expecting at all.
I was also surprised to see that enrollment among seniors inched up ever so slightly (about 0.4%, or 1,500 people). Huh.
Next up: Premiums, Advance Premium Tax Credits (APTC) and Cost Sharing Reduction (CSR) assistance.
Nationally, the average unsubsidized premiums for 2026 exchange-based Open Enrollment Period enrollees are $741/month, up $122/month or 19.7% from last year.
This is a smaller average gross increase than the 25.5% I had projected last fall...for two rather obvious reasons, which I try to make clear every year:
Now it's time to move on to the actual demographic breakout of 2026 Open Enrollment Period (OEP) Qualified Health Plan (QHP) enrollment.
First up: Breaking out new enrollees vs. existing enrollees who either actively re-enroll in an exchange plan for another year or who passively allow themselves to be automatically renewed into their current plan (or to be "mapped" to a similar plan if the current one is no longer available).
Nationally, 15.6% of all exchange QHP enrollees were new this year. The other 84.4% are current enrollees who signed up for another year.
Fortunately, more enrollees took my advice and actively re-enrolled this year (46.3% vs just 39% last year). Unfortunately, 38.1% still allowed themselves to be passively auto-renewed. Those are the ones who, in many cases, were likely hit with massive sticker shock as they were auto-renewed into a plan which probably had dramatically higher premiums due to the enhanced tax credits expiring...over 8.8 million enrollees nationally.
When I last checked in on the official 2026 ACA Open Enrollment Period (OEP) data from the Centers for Medicare & Medicaid Services (CMS), they had published the "top line" enrollment numbers for each state, including final numbers for the 30 states hosted via the federal ACA exchange (HealthCare.Gov) and semi-final data for the remaining 20 states (+DC) which operate their own ACA exchanges.
I've repeatedly warned that the final, official CMS 2026 OEP report--which includes far more detailed demographic data including breakouts by metal level, income brackets, financial assistance and so forth likely wouldn't be published until late April or early May based on last year when it wasn't published until May 11th.
Well, it turns out they moved that up substantially after all: The final 2026 OEP Public Use File was just uploaded at CMS today...and while there hasn't been any formal press release published yet, I have a copy regardless.
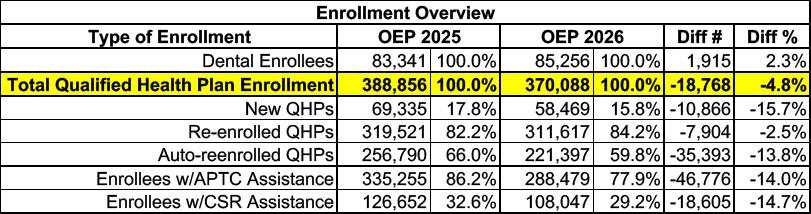
Here's the overview of Virginia ACA exchange enrollment over the course of OEP 2026 vs. 2025. Stand-alone dental plan enrollment is up 2.3%, which is nice, but overall major medical plan (Qualified Health Plan, or QHP) enrollment dropped by nearly 19,000 people, or 4.8% year over year.
There's also 14% fewer enrollees receiving federal tax credits than last year (nearly 47,000 people), while another 15% lost Cost Sharing Reduction assistance (CSR).
Last month I posted a massive3-partseries of articles which looked at nearly 3 dozen changes being proposed by the Trump Regime's Centers for Medicare & Medicaid Services (CMS) to how the Affordable Care Act will be administered starting this fall (for the 2027 plan year).
The changes ranged from the mundane (for instance, one provision simply says that the per enrollee user fees paid by insurance carriers to HHS to pay for HealthCare.Gov's operations will remain the same as they are this year) to the devastating (up to 1.5 million legally-present immigrants who were previously eligible for ACA tax credits, including victims of domestic abuse and human trafficking, either already are or will soon become ineligible for financial assistance).
Centers for Medicare & Medicaid Services Approves New York’s Request to Transition Back to Basic Health Program Authority
Approximately 450,000 New Yorkers Will Become Ineligible for the Essential Plan Beginning July 1, 2026, and Will Instead Be Eligible for Qualified Health Plans
ALBANY, N.Y. (March 23, 2026) - The New York State Department of Health provided an update following federal approval from the Centers for Medicare & Medicaid Services (CMS) of the State’s request to terminate its Section 1332 State Innovation Waiver and return to Basic Health Program (BHP) authority.
The transition preserves Essential Plan coverage for approximately 1.3 million New Yorkers with incomes below 200 percent of the federal poverty level.
A few weeks ago I noted that the first hard data on effectuated ACA marketplace enrollment (as opposed to how many people selected plans) had started to come in from a handful of states...Maryland and Massachusetts in particular. While the data is still sparse, the early trendlines are already starting to show up:
Medicare Advantage (technically "Medicare Part C" & originally called "Medicare+Choice") is a type of health plan in the United States offered by private companies as part of the original Social Security Act of 1965 that created Medicare. It permits a private insurance option that wraps around traditional Medicare. Medicare Advantage plans attempt to fill some coverage gaps and offer alternative coverage options.
Under Part C, Medicare pays a plan operator a fixed payment for each enrollee. The operator then pays for their medical expenses. Traditional Medicare directly compensates providers on a fee-for-service basis. Plans are offered by integrated health delivery systems, labor unions, non profit charities, and health insurance companies, which may limit enrollment to specific groups of people (such as union members).
A health savings account (HSA) is a tax-advantaged medical savings account available to taxpayers in the United States who are enrolled in a high-deductible health plan (HDHP). The funds contributed to an account are not subject to federal income tax at the time of deposit. Unlike a flexible spending account (FSA), HSA funds roll over and accumulate year to year if they are not spent. HSAs are owned by the individual...
...HSA funds may be used to pay for qualified medical expenses at any time without federal tax liability or penalty. Beginning in early 2011 over-the-counter medications could not be paid with an HSA without a doctor's prescription, although that requirement was lifted as of January 1, 2020. Withdrawals for non-medical expenses are treated very similarly to those in an individual retirement account (IRA) in that they may provide tax advantages if taken after retirement age, and they incur penalties if taken earlier.
For months now I've been warning that the initial data published about the 2026 ACA enrollment would likely massively underestimate just how ugly things were in terms of both effectuated enrollment as well as how comprehensive the coverage would be for those who did enroll.
Back in December, when Open Enrollment was still going on, I noted that regardless of what the official number of Americans who selected an exchange plan during Open Enrollment was, the actual number of those who would have effectuated coverage over the course of the year would likely be far lower:
So, what will this graph look like for 2026?
...IF that's what ends up happening, it would look something like the following:
In U.S. politics, the Hyde Amendment is a legislative provision barring the use of federal funds to pay for abortion, except to save the life of the woman, or if the pregnancy arises from incest or rape. Before the Hyde Amendment took effect in 1980, an estimated 300,000 abortions were performed annually using federal funds.
HealthSource RI Open Enrollment 2026 closes with falling enrollment trend
Mar 9, 2026
PROVIDENCE, RI – HealthSource RI (HSRI) concluded its annual Open Enrollment (OE) period January 31, with enrollment totals and the mix of plan selections bearing out expectations, as customers faced increased monthly costs upon the expiration of enhanced federal premium tax credits. Individual and Family enrollments totaled 38,557 during this Open Enrollment, a 10-percent decline from the record-high close of OE2025 (42,695). Overall enrollment decreased by 20% from year-end (48,060) to the end of OE, a highly unusual development, as the marketplace has recorded growth nearly every year in that same span.
Over the past week or so, a few more state-based ACA exchanges have quietly published their final, official 2026 ACA Open Enrollment Period data, including Connecticut (157,246 plan selections), New Jersey (509,192), the District of Columbia (16,053) and Virginia (370,088). With these updates, practically all of the official 2026 OEP topline numbers are now filled in except for the following:
About a month ago, I once again reiterated that the official year over year ACA Open Enrollment Period plan selection drop from OEP 2025 to OEP 2026, which currently stands at around 1.26 million people (23.06M in 2026 vs. 24.32M in 2025) was incredibly misleading for a number of reasons:
Not only are there always some people who never have their enrollment effectuated in the first place due to either the policyholder actively cancelling their policy before it even begins or having it terminated by the carrier due to them not paying their first monthly premium, but that effectuated enrollment can vary widely from month to month due to the "churn" of people either starting or ending exchange coverage.